

Translate this page into:
T1 contrast versus fluid-attenuated inversion recovery contrast technique for evaluation of cerebral tuberculosis
 , Joe Vimal Raj1, Pugazhendhi Sambath1, Avinesh Varadane1
, Joe Vimal Raj1, Pugazhendhi Sambath1, Avinesh Varadane1

*Corresponding author: Balavaitheeswar Ramalingam, Department of Radiodiagnosis, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India. ahilanbala20@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ramalingam B, Padmanaban E, Vimal Raj J, Sambath P, Varadane A. T1 contrast versus fluid-attenuated inversion recovery contrast technique for evaluation of cerebral tuberculosis. Glob J Health Sci Res 2023;1:146-9.
Abstract
Objectives:
T2-weighted (T2W) fluid-attenuated inversion recovery (FLAIR), a traditional magnetic resonance imaging (MRI) technique, is regarded as one of the most effective methods for examining brain disorders. The identification of brain pathologies can be significantly aided by T2 FLAIR and T1 post-contrast imaging. However, lesion enhancement is occasionally inconspicuous on T1-weighted image. Hence, for the evaluation of brain disorders, a MRI approach known as FLAIR contrast would combine the benefits of T2W FLAIR with contrast-enhancement on a single picture.
Material and Methods:
After obtaining clearance from the Institution’s Ethics Committee, contrast-enhanced MRI (CE-MRI) brain of 20 patients was taken for the study. CE-MRI was performed using 1.5 Tesla Intera PHILIPS with intravenous administration of gadolinium at approximately 0.1 mL/kg/body at a rate of 10 mL/15 s.
Results:
This study showed a better appreciation of lesion conspicuity when compared to prior T1 contrast images. However, there was no significant difference in the number of lesions, lesion extension, and degree of contrast-enhancement on comparison with T1 contrast images.
Conclusion:
T1 FLAIR contrast shows a better appreciation of lesion conspicuity when compared to T1 contrast images. Post-contrast FLAIR imaging is a valuable adjunct to post-contrast T1W imaging and effectively delineates cerebral tubercular pathologies. However, T1 FLAIR cannot be used as a replacement for conventional T1 fat saturated post-contrast imaging.
Keywords
T1 contrast
T2 fluid-attenuated inversion recovery
T1 fluid-attenuated inversion recovery contrast
Cerebrum
Tuberculosis

INTRODUCTION
The fluid-attenuated inversion recovery (FLAIR) approach uses an inversion recovery pulse sequence with an inversion duration that, when used with long-TE T2-weighted (T2W) imaging, effectively nullifies signals from the CSF. The mild T1 effect of the FLAIR sequence is responsible for contrast enhancement on these heavily T2W images. FLAIR imaging of the brain is sensitive for detecting parenchymal lesions and is also promising in evaluating cerebral tubercular pathologies. To diagnose brain diseases, magnetic resonance imaging (MRI) contrast termed FLAIR contrast combines the drawbacks of T2W FLAIR contrast in a single image.[4,8] Our purpose was to compare post-contrast T1-weighted (T1W) and FLAIR images in evaluating cerebral tubercular pathologies.
MATERIAL AND METHODS
This study was carried out in the Department of Radiodiagnosis, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India. It is a hospital based prospective study. After obtaining clearance from the Institute’s Ethics Committee, 20 cases who were referred to the department of radiodiagnosis for contrast-enhanced MRI (CE-MRI) brain during the period of August 2021–October 2022 were analyzed. Patients of all ages and both sexes were included in the study. CE-MRI was performed using 1.5 Tesla Intera PHILIPS with intravenous administration of gadolinium at approximately 0.1 mL/kg/body at a rate of 10 mL/15 s. T1 FLAIR contrast sequence was imaged for the patients who had ring enhancing lesions on prior T1 contrast images. Images were obtained in axial and sagittal sections. After acquiring the images, the enhancement pattern and imaging features of T1 contrast and FLAIR contrast technique were compared. The results obtained were calculated and tabulated.
Study design
This is a hospital-based and prospective study.
Inclusion criteria
All patients of either sex who had ring enhancing lesions on T1 contrast images and were imaged for FLAIR contrast sequence were included in the study.
Exclusion criteria
The following criteria were excluded from the study:
Patients with metallic prosthesis and cochlear implants
Patients with claustrophobia
Patients with pacemakers
Patient MR-incompatible prosthetic heart valves.
RESULTS
The total number of patients included in the study was 20, which includes 14 males and six females [Figure 1]. The median age of participants is 45 years, with age ranging from 15 to 75 years [Table 1].
| Range | No. of patients |
|---|---|
| 15–30 | 2 |
| 31–45 | 4 |
| 46–60 | 10 |
| 61–75 | 4 |
| Total | 20 |
- Gender distribution.
FLAIR contrast technique for evaluation of cerebral tuberculosis was imaged. In our study, there were no significant differences between T1 and FLAIR contrast images on the basis of number of lesions, lesion extension, and degree of enhancement. There was a significant difference in lesion conspicuity when compared to T1 contrast images. Fifteen out of 20 patients with cerebral tuberculosis showed significant lesion conspicuity on comparison with T1 contrast images.
| Description | FLAIR superior to T1C+ |
FLAIR equal to T1C+ |
FLAIR inferior to T1C+ |
|---|---|---|---|
| New lesions | - | 20 | - |
| Lesion conspicuity | 10 | 5 | 5 |
| Degree of contrast enhancement | - | 12 | 8 |
FLAIR: Fluid-attenuated inversion recovery
DISCUSSION
Central nervous system tuberculosis results from either hematogenous spread from distant systemic infection or direct extension from local infection. Its manifestation includes meningitis, pachymeningitis, tuberculoma formation, non-caseating granuloma, caseating granuloma, caseating granuloma with central liquefaction, and calcified granuloma are the various stages of tuberculous granuloma.
T1 post-contrast study showed a significant role in differentiation of various intracranial tuberculoma stages. However, lesion enhancement is occasionally inconspicuous on T1-weighted image (T1WI). Despite being often used, FLAIR sequences also exhibit modest T1W contrast, which causes the contrast amplification.[9] High contrast for cerebral tuberculosis may be seen in high-isotropic resolution FLAIR images acquired at 1.5T, making it well suited to investigate the relationship between cerebral tuberculosis in a clinical setting.
Contrast-enhanced FLAIR (CE-FLAIR) imaging does not demonstrate enhancement in the normal vascular structures or meninges that can be confused with abnormal meningeal enhancement on CE-T1WI.[5,6] In addition, due to its extreme sensitivity to minimal modification of the CSF composition, CE-FLAIR is more sensitive to lower gadolinium concentrations.
Our study showed higher percentage of lesion conspicuity when compared to T1 contrast images [Figure 2]. Similar results were exhibited in a study conducted by Sati et al.[1] stating high-isotropic-resolution FLAIR* images yield high contrast for white matter lesions. There was no significant difference in number of lesions, lesion extension, and degree of enhancement [Figure 3]. Another similar results were exhibited in a study conducted by Mustafa et al.[2] stating CE-FLAIR imaging should be used as a routine or adjunctive sequence to CE-T1WI to enhance early detection and increase the diagnostic confidence in MRI examination of different brain pathological conditions.[3,7]
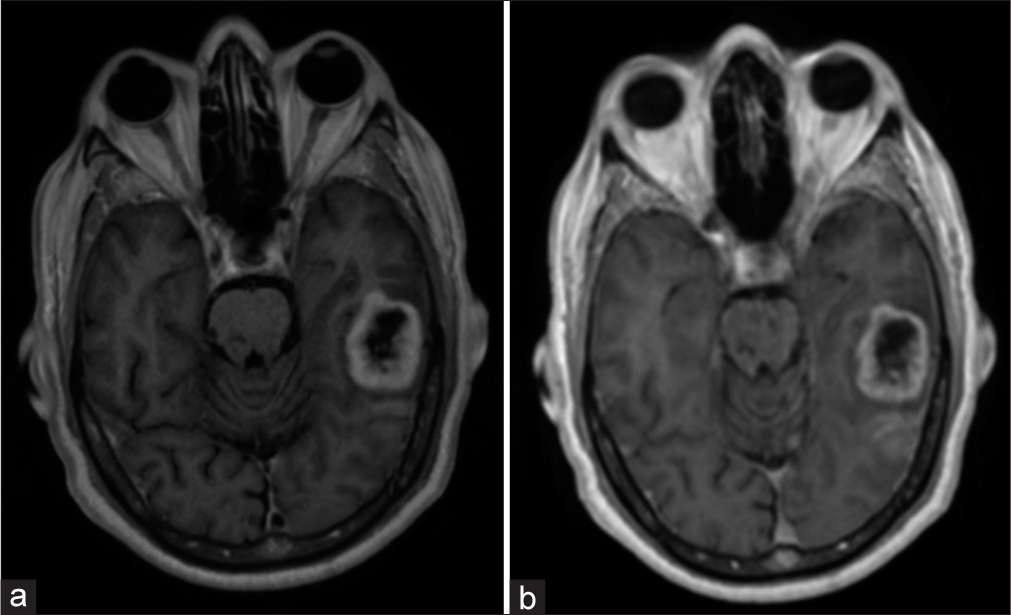
- 66/M with seizures. (a) contrast-enhanced magnetic resonance imaging brain fluid-attenuated inversion recovery contrast images show the increased conspicuity of the lesion when compared to T1 contrast images (b).
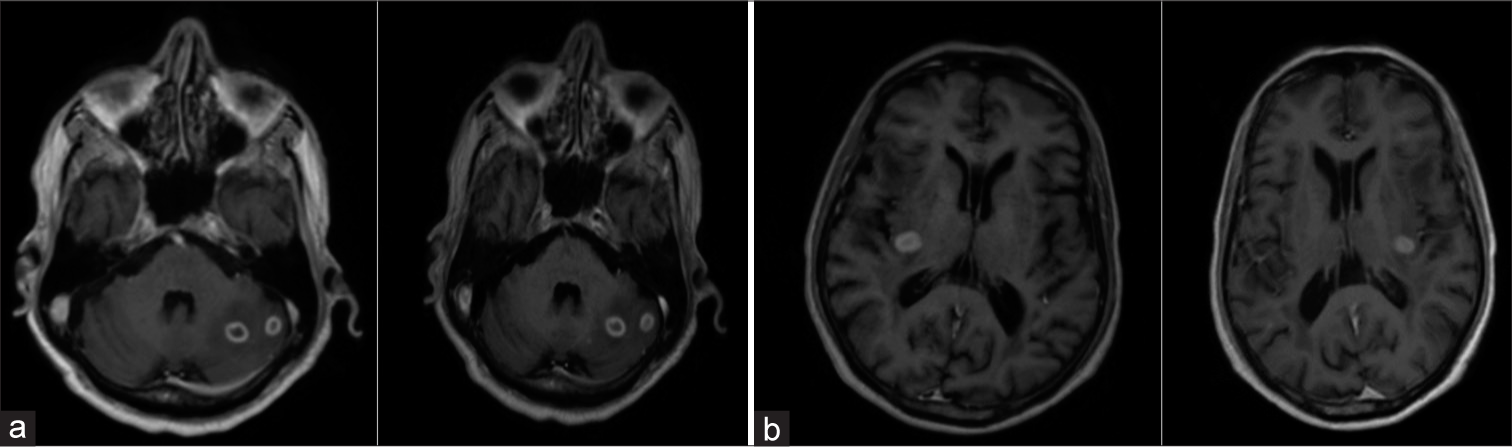
- 60/M with seizures. (a) contrast-enhanced magnetic resonance imaging fluid-attenuated inversion recovery contrast images show the lesion conspicuity was increased, however, there was no significant difference in delineation in new lesions, lesion extension, and degree of contrast enhancement when compared to T1 contrast images (b).
Hence, T1 FLAIR contrast imaging of the brain is sensitive for evaluating cerebral tubercular pathologies and can be used as an adjunctive sequence to contrast-enhanced T1W imaging.
CONCLUSION
CE-FLAIR imaging has many advantages for evaluating cerebral pathologies. CE-FLAIR imaging can be used as an adjunctive sequence to CE-T1WI in equivocal cases to increase the diagnostic confidence and improve patient care. Hence, routine use of FLAIR imaging before and after the administration of contrast is particularly useful for delineating cerebral tuberculosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- FLAIR*: A combined MR contrast technique for visualizing white matter lesions and parenchymal veins. Radiology. 2012;265:926-32.
- [CrossRef] [PubMed] [Google Scholar]
- Role of contrast-enhanced FLAIR MRI in diagnosis of intracranial lesions. Egypt J Neurol Psychiatr Neurosurg. 2021;57:1-2.
- [CrossRef] [Google Scholar]
- Diagnostic value of contrast-enhanced fluid-attenuated inversion recovery MR imaging of intracranial metastases. AJNR Am J Neuroradiol. 2004;25:761-5.
- [Google Scholar]
- Comparison of T1-Post and FLAIR-Post MRI for identification of traumatic meningeal enhancement in traumatic brain injury patients. PLoS One. 2020;15:e0234881.
- [CrossRef] [PubMed] [Google Scholar]
- The value of contrast-enhanced FLAIR magnetic resonance imaging in detecting meningeal abnormalities in suspected cases of meningitis compared to conventional contrast-enhanced T1WI sequences. Egypt J Radiol Nucl Med. 2020;51:1-6.
- [CrossRef] [Google Scholar]
- Postcontrast fluid-attenuated inversion recovery (FLAIR) sequence MR imaging in detecting intracranial pathology. Radiol Res Pract. 2020;2020:8853597.
- [CrossRef] [PubMed] [Google Scholar]
- Added value of delayed post-contrast FLAIR in diagnosis of metastatic brain lesions. Egypt J Radiol Nuclear Med. 2022;53:1-2.
- [CrossRef] [Google Scholar]
- Contrast-enhanced FLAIR (fluid-attenuated inversion recovery) for evaluating mild traumatic brain injury. PLoS One. 2014;9:e102229.
- [CrossRef] [PubMed] [Google Scholar]
- Build-A-FLAIR: Synthetic T2-FLAIR Contrast Generation through Physics Informed Deep Learning United States of America: Cornell University; 2019.
- [Google Scholar]




