

Translate this page into:
Relationship of the severity of talipes equinovarus and age of presentation to time of correction: A focus on Dimeglio scoring
 , Omolade Ayoola Lasebikan2, Joseph Asuquo3, Obaji Etaba Akpet4, Best Joseph Asuquo5, Ehiosun Jude Aigbomian6
, Omolade Ayoola Lasebikan2, Joseph Asuquo3, Obaji Etaba Akpet4, Best Joseph Asuquo5, Ehiosun Jude Aigbomian6

*Corresponding author: Joseph Asuquo, Department of Orthopaedics and Trauma, University of Calabar, Calabar, Nigeria. itansuq@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Ubiomo ED, Lasebikan OA, Asuquo J, Akpet OE, Asuquo BJ, Aigbomian EJ. Relationship of the severity of talipes equinovarus and age of presentation to time of correction: A focus on Dimeglio scoring. Glob J Health Sci Res 2023;1:116-20.
Abstract
Objectives:
The Ponseti method is the mainstay of treatment of congenital talipes equinovarus deformity. This study aims to assess the relationship between the severity of the clubfoot deformity and the time it takes to correct the deformity using Dimeglio scoring system (DSS) with Ponseti protocol.
Material and Methods:
A prospective observational study carried out for 15 months at the outpatient department of the National Orthopedic Hospital Enugu. Data collected included age at presentation, sex, laterality, grade of deformity, number of casts, and time to correction before the commencement of bracing. Those selected were clinically assessed using the DSS. Data obtained were analyzed using SPSS version 22.0. The association between time, the number of casts to correction, age of presentation, and severity to the time of correction of deformity was also determined.
Results:
A total of 70 patients (116 feet) were recruited for the study. The mean age at presentation was 21 weeks with a male-to-female ratio of 3:2. The mean DSS at presentation was 10.72. The mean number of casts required to achieve correction was 5, with the last cast left in place for 3 weeks, which gave a mean correction time of 7 weeks. Severe deformity required more cast for correction. There is a weak relationship between age and time to correction.
Conclusion:
Increase in the severity of the clubfeet was associated with longer correction time and a weak correlation with age at presentation. Dimeglio scoring is an effective, grading, and monitoring system.
Keywords
Clubfoot
Severity
Time to correction
Dimeglio scoring

INTRODUCTION
Congenital talipes equinovarus (CTEV), also known as clubfoot, is an aggregation of deformities of the ankle and foot. It consists of forefoot adduction, cavus of the midfoot, varus of the heel, and equinus of the ankle.[1] Although club foot is a broader term encompassing other deformities, in this study, both terms will be used interchangeably. The deformity may be present at birth (primary or congenital club foot). Primary clubfoot can be either idiopathic clubfoot (etiology is unknown and not associated with deformities in other parts of the body) or syndromic clubfoot (arises as part of many neurological or neuromuscular disorders such as spina bifida).[2,3] Clubfoot may be acquired later in life, also known as secondary clubfoot. The primary idiopathic type is relatively common, with an average incidence of 1–2/1000 births, 50% of which are bilateral.[2,3] Its exact cause is yet to be determined, though several theories have been put forward in an attempt to explain it.[1] The diagnosis of idiopathic CTEV is clinical.[4,5] Several scoring systems have been developed to assess the severity of clubfoot deformity; one of the common methods of determining the severity of the deformity is the Dimeglio scoring system (DSS).[6,7] This system classifies the deformity into benign, moderate, severe, and very severe foot deformity based on scores given to several parameters which include equinus, varus, supination, adduction, posterior crease, medial crease, cavus, and deviant muscle function. The minimum score is 0, while the maximum score is 20.[7] In cases of bilateral deformity, each limb is scored independently. The Dimeglio score is detailed and reproducible and has to be repeated on each visit to the clinic.[7]
Parents and caregivers of patients with clubfoot deformity often show immense anxiety and worry over the duration of casting/hospital visits in the course of treatment. This is made worse by the poor socioeconomic status of some of these parents. Studies done so far have proven that the Ponseti method is effective in the treatment of clubfoot,[8,9] but some of these studies have not been able to ascertain the extent to which certain factors such as the severity of the deformity at presentation and the age at presentation affect the time to correction of the deformity. Therefore, this study aims to evaluate the relationship between the severity of talipes equinovarus using the DSS to the time and number of casts it takes to correct the deformity using the Ponseti method.
MATERIAL AND METHODS
The study was a prospective observational hospital-based study, carried out at the Outpatient Department (OPD) of the National Orthopedic Hospital Enugu, a regional orthopedic center located in South-East Nigeria for a period of 15 months, from January 1, 2018, to March 31, 2019. It was focused on children that were <4 years of age, who presented with idiopathic CTEV deformity of one or both feet with no previous history of surgical intervention and were treated by the Ponseti method for management of clubfoot.
These patients were consecutively recruited for the study in the first 12 months, while each patient was followed up for a period of 3 months, for the duration of castings ± tenotomy until full correction of the deformity was achieved. Patients who refused to give consent and those with syndromic clubfoot, secondary clubfoot deformity, complex clubfoot, and relapsed clubfoot were excluded from the study.
Ethical clearance was obtained from the Hospital Ethics Committee before the study was commenced. Since the patients were minors, the parents or the caregivers of patients selected for the study were educated in their own local dialect on the procedure, counseled on the reason for the study, the anonymity of patients’ identity were preserved and the freedom to either accept or decline participation in the study at any time. A written informed consent in simple terms was obtained from the parent or caregiver of each participant before his or her enrollment into the study.
The patients for the study were recruited at the OPD Clubfoot Clinic, after the diagnosis of idiopathic CTEV was made by the attending surgeon. The patient’s feet were examined, the diagnosis confirmed, and the severity of the deformity was assessed using the DSS. A general examination was also done, to rule out other congenital or acquired deformities. All manipulation and casting were performed by the authors. Manipulation and casting were done every 7 days at the clubfoot clinic. Above knee POP casts were applied after application of soft ban to reduce the risk of development of pressure sore.
The foot was manipulated to correct the deformities according to the Ponseti protocol. At the first visit/session, the forefoot was supinated to align it with the hind-foot apparently increasing the deformity. Thereafter, an above knee POP cast was applied to the limb with the foot in the new position and with the knee flexed at 90°. From the second visit onward, gradual abduction of the forefoot and the midfoot while reducing the talonavicular subluxation/ dislocation with thumb pressure over the head of the talus was carried out over weeks. Each new corrected position of the foot maintained in above knee POP cast with the knee in 90° of flexion until the foot attained 60° of abduction. This position was also maintained with a POP cast keeping the knee in 90° of flexion to avoid losing the correction. Tarsal coupling ensures equinus correction with progressive abduction. Any residual equinus deformity was corrected by gradual dorsiflexion of the foot after full abduction of about 60 degrees had been achieved.
Once the forefoot and the midfoot deformities were corrected, but the maximum dorsiflexion achieved was <10° percutaneous. Achilles tenotomy was performed in the clinic under local anesthesia. With or without performing tenotomy, a final above knee cast was applied to the limb(s) with the knee in 90° of flexion, for a period of 3 weeks before it was removed. A final Dimeglio score of the foot was obtained before the application of foot abduction orthosis. The age of the patient at first presentation was noted and the duration of treatment/number of manipulation and castings required to achieve correction of the deformity was also noted.
Data were collected using a well-designed and structured, personally administered pro forma. Each patient enrolled for the study had his/her data filled into the pro forma. Data collected included the biodata – age at presentation and sex of the patient and the phone number of caregiver for follow-up. The foot/feet affected and the Dimeglio score at the first presentation was documented. After the removal of the final cast, the Dimeglio score and the number of casts used to correct the deformity were documented. Patients were grouped by the Dimeglio scores and compared with the number of casts and time required for deformity correction. Patients were also grouped by age and compared with the number of casts used and the time taken for deformity correction.
Data analysis was carried out with electronic computer software, IBM Statistical Package for Services Solution version 22.0 (IBM SPSS version 22.0).
RESULTS
A total of 70 patients with 116 feet were recruited. The mean age (weeks) at presentation was 21.47 ± 4.42 with an age range of 1–192 weeks. Majority of the patients were <52 weeks of age (67.1%).
The mean Dimeglio score was 10.72 (S.D. 4.09) with a range of 1.50–18.00. Majority of the patients (70.7%) presented with moderate-to-severe grades of deformity [Figure 1].
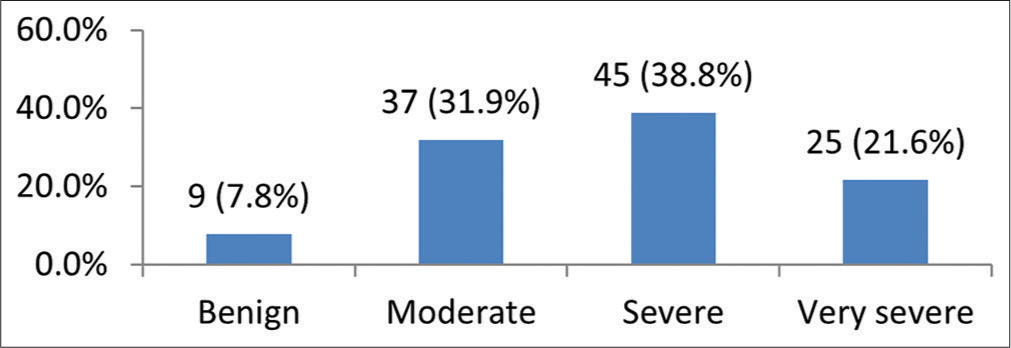
- Severity of clubfoot deformity.
The mean number of casts was 5.28 ± 2.05 (range 2–9) to achieve correction [Table 1].
| No. of cast(s) | Duration of casting | Frequency | Percent |
|---|---|---|---|
| 2 | 4 | 11 | 9.5 |
| 3 | 5 | 20 | 17.2 |
| 4 | 6 | 11 | 9.5 |
| 5 | 7 | 18 | 15.5 |
| 6 | 8 | 20 | 17.2 |
| 7 | 9 | 20 | 17.2 |
| 8 | 10 | 8 | 6.9 |
| 9 | 11 | 8 | 6.9 |
The mean duration of treatment in weeks was 7.28 ± 2.05 [range: 4–11].
The mean number of casts significantly increased with severity (F = 31.831, P < 0.001). However, Duncanmultiple comparison tests show that the severe and very severe groups required similar mean number of casts [Table 2].
| Benign Mean±SD |
Moderate Mean±SD |
Severe Mean±SD |
Very severe Mean±SD |
F | P-value | |
|---|---|---|---|---|---|---|
| No. of casts | 2.67±0.50 | 3.89±1.85 | *6.07±1.48 | *6.84±1.25 | 31.831 | <0.001 |
SD: Standard deviation. *Duncan multiple comparison test indicating means not significantly different
The duration of treatment significantly increased with severity (F = 31.831, P < 0.001). However, Duncan multiple comparison tests show that the severe and very severe groups had similar duration of treatment to achieve correction [Table 3].
| Benign Mean±SD |
Moderate Mean±SD |
Severe Mean±SD |
Very severe Mean±SD |
F | P-value | |
|---|---|---|---|---|---|---|
| Duration of treatment | 4.67±0.50 | 5.89±1.85 | *8.07±1.48 | *8.84±1.25 | 31.831 | <0.001 |
SD: Standard deviation. *Duncan multiple comparison test indicating means not significantly different
Forty-six patients (65.7%) had bilateral clubfoot deformity, while 24 patients (34.3%) had unilateral clubfoot deformity.
The tenotomy rate was 58%.
DISCUSSION
The DSS is one of the scoring systems being used to grade clubfoot deformity for the purpose of treatment and follow-up. It is reliable, reproducible, and effective. Our study reveals that the higher the initial Dimeglio score the more the number of cast needed to achieve correction, the correlation was strong and statistically significant. This finding is similar to that reported by several authors in other climes and settings,[10,11] but a study has a slightly different opinion. Their correlation was weak.[12]
There was a positive correlation between the age at initiation of treatment and the number of cast. The higher the age at presentation, the higher the number of cast needed to achieve correction. This finding was similar to that reported by some authors.[13,14] while others have different opinion.[10] This is largely a chance observation because the number of cast depends largely on the initial Dimeglio score at presentation.
The mean number of cast required to achieve correction was similar to that reported by Romanian, Bangladesh, and USA studies. Their mean number of cast was 4, 5, and 5, respectively. These findings were comparable to other studies in Nigeria that used a different scoring system. This affirms the reproducibility of this scoring system[11,15,16]
From our study, the mean score and range for our patients was similar to that reported by both Romanian and an Italian study (10.7 and 12.7 points, respectively, the range was 4–18 and 6–19 points, respectively).[10,15]
The age at presentation in our study was lower than that reported by other Nigerian study, even though the majority of their patients were <24 weeks old.[17] This can be due to the increased awareness of the successful treatment of clubfoot without surgery. However, a local study suggested otherwise, although most of the respondents were primigravidas.[18]
From our study, the tenotomy rate using the DSS was relatively lower than that reported by another local study.[17] This can be due to lower age at presentation and the small sample size.
The strength of the study is that DSS is not popular in our country and this is the first study to demonstrate that it can be effectively used compared to the Pirani scoring system. A larger cohort is required to ascertain its efficiency and effectiveness.
The weakness of this study is in the sample size and it is a hospital-based study.
CONCLUSION
This study reveals that increase in severity of the deformity as shown by the Dimeglio score was associated with longer correction time. There was a weak association between age at presentation and time to correction. The DSS can be used for grading, treating, and monitoring of clubfoot.
Declaration of patient consent
The Institutional Review Board (IRB) permission obtained for the study.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Descriptive epidemiology and predisposing factors to idiopathic talipes equinovarus in South South Nigeria. J Public Health Epidemiol. 2016;8:147-51.
- [CrossRef] [Google Scholar]
- Increasing incidence of clubfoot in the county of Frederiksbog Denmark. Ugeskr Laeger. 1998;160:4215-7.
- [Google Scholar]
- Genetic and environmental factors in the etiology of talipes equinovarus. Clin Orthop. 1972;84:9-13.
- [CrossRef] [PubMed] [Google Scholar]
- Increasing incidence of clubfoot with higher population density; incidence and geographical variation in Denmark over a 16 year period-an epidemiological study of 936,525 births. Acta Orthop. 2006;77:839-46.
- [CrossRef] [PubMed] [Google Scholar]
- A South Australian population based study of congenital talipes equinovarus. Peadiatr Perinat Epidemiol. 2005;19:227-37.
- [CrossRef] [PubMed] [Google Scholar]
- The classification of congenital talipes equinovarus. J Bone Joint Surg Br. 2002;84:1020-4.
- [CrossRef] [PubMed] [Google Scholar]
- Initial treatment of congenital idiopathic clubfoot: Prognostic factors. Orthop Traumatol Surg Res. 2016;102:1081-5.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital talipes equinovarus (CTEV) In: Essential Orthopaedics Vol 25. (4th ed). New Delhi: Jaypee Brothers Medical Publishers Ltd; 2011. p. :203-11.
- [CrossRef] [Google Scholar]
- Comparison of Dimeglio and Pirani score in predicting number of casts and the need for tenotomy in clubfoot correction using the Ponseti method. Int Orthop. 2018;42:2429-36.
- [CrossRef] [PubMed] [Google Scholar]
- Dimeglio score predicts treatment difficulty during Ponseti casting for isolated clubfoot. J Pediatr Orthop. 2019;39:402-5.
- [CrossRef] [PubMed] [Google Scholar]
- Clubfoot classification: Correlation with Ponseti cast treatment. J Pediatr Orthop. 2010;30:695-9.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of idiopathic clubfoot using Ponseti method: Minimum 2-year follow-up. J Pediatr Orthop Part B. 2007;16:98-105.
- [CrossRef] [PubMed] [Google Scholar]
- Ponseti technique for the management of congenital talipes equinovarus in a rural set-up in India: Experience of 356 patients. Children (Basel). 2018;5:49.
- [CrossRef] [PubMed] [Google Scholar]
- Outcome of management of congenital idiopathic clubfoot by Ponseti technique. Bang Med J Khulna. 2015;48:11-5.
- [CrossRef] [Google Scholar]
- Frequency of percutaneous achilles tenotomy in the treatment of idiopathic clubfoot using Ponseti technique. Niger J Med. 2018;27:163-7.
- [CrossRef] [Google Scholar]
- Awareness and knowledge of congenital clubfoot among antenatal clinic attendees in Calabar. Niger Qt J Hosp Med. 2021;31:32-8.
- [Google Scholar]




