

Translate this page into:
Longitudinal tooth fracture indicating a questionable prognosis for an endodontist

*Corresponding author: Ravinder Nath Bansal, Department of Hospital Administration, Guru Gobind Singh Medical Hospital, Faridkot, Punjab, India. rnbansal@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta S, Garg R, Bansal R. Longitudinal tooth fracture indicating a questionable prognosis for an endodontist. Glob J Health Sci Res. 2025;3:6-10. doi: 10.25259/GJHSR_3_2024
Abstract
Introduction and Objectives:
Longitudinal fracture or vertical fracture of a tooth occurs at any level in the root and extends vertically. It has a high incidence of occurrence in the first molars. The most frequent sites to occur are the buccolingual surface and proximal surfaces of teeth. The etiology of fracture involves different factors in endodontically treated and non-endodontically treated teeth. Longitudinal fractures become the most challenging to diagnose and treat. This paper reviews these aspects of challenges and discusses the advantages and limitations of dental materials used for the treatment.
Review Methods:
PubMed and Google Scholar databases were searched for articles on longitudinal tooth fractures between 2007 and 2022. The 16 current articles were selected.
Brief Description of the State of Knowledge:
As per the review of the literature, longitudinal fracture of the tooth is the most common fracture to occur due to excessive forces on the root canal-treated tooth. This occurs in endodontically treated teeth due to long-term application of calcium hydroxide, cracks caused during root canal preparation extended by the pressure of root canal obturation, and in non-endodontically treated teeth due to cyclic and heavy masticatory stress, and habitual chewing of hard food especially in males.
Summary:
Functional and esthetic outcomes following longitudinal fracture treatment are important considerations in the case of anterior teeth. Longitudinal fracture or vertical fracture of a tooth occurs mostly in the first molars. It is crucial to identify and manage actors for good prognosis, as restoration at a time can reduce fracture extension prevent microleakage.
Keywords
Challenges
Endodontic treatment
Longitudinal fracture
Vertical fracture

INTRODUCTION
Longitudinal fracture is also known as vertical fracture of a tooth. It means a fracture of the tooth, which initiates at any level in the root and extends along the root in a vertical direction.[1-3] This type of fracture changes with time or, in other words, extends with time as compared to fracture due to trauma. It mostly occurs in premolars with a higher incidence followed by first molars. It commonly involves a buccolingual surface and may include a proximal surface. Longitudinal fractures are of several types depending on the severity of fracture,[1] as shown in Figure 1.
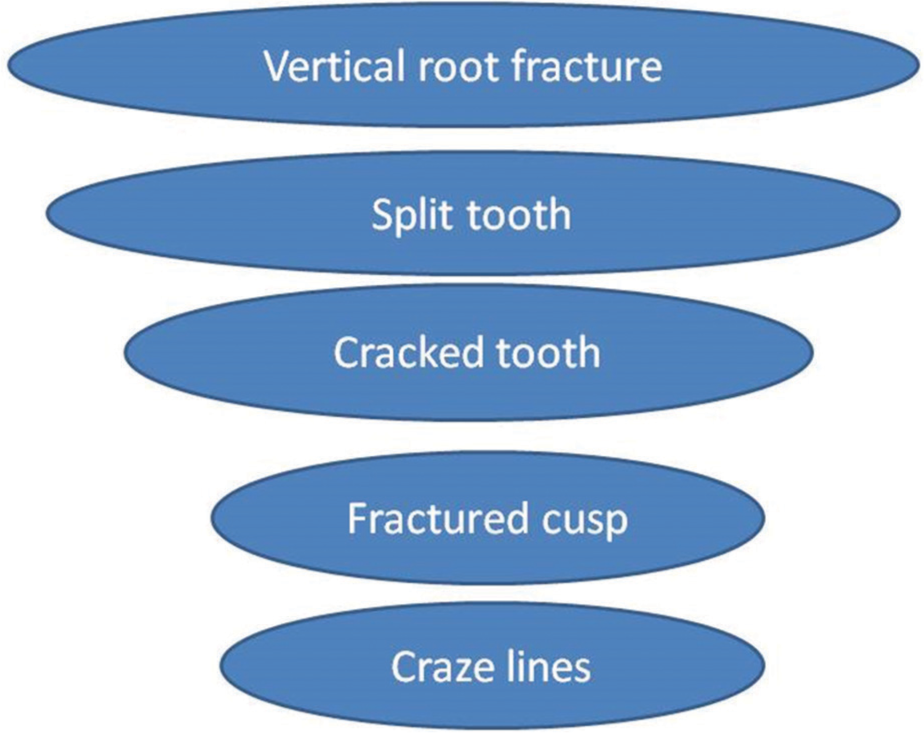
- Types of longitudinal fracture from least to severe.
ETIOLOGY OF LONGITUDINAL FRACTURE
There are several reasons for longitudinal (vertical) fractures to occur[4] mentioned in Table 1.
| In endodontically treated teeth |
|
| In non-endodontically treated teeth |
|
CHALLENGES IN THE DIAGNOSIS OF LONGITUDINAL FRACTURE
These types of tooth fractures are not rare and are most challenging for a dental surgeon. On the one hand, some cases are manageable; on the other hand, some are near to extraction. It may be complete or incomplete. In endodontics, it is the most common reason for failure and reason for extraction.[1]
Longitudinal fractures of tooth are difficult to diagnose and manage without any expert opinion. Why this incorrect diagnosis or difficulty in diagnosis arises is a critical factor to be considered in dental practice. Inappropriate knowledge regarding the type of fracture and characterization of severity of fracture are among these factors.[1]
Longitudinal fracture develops slowly in a timely manner, mostly unnoticed by the patient until clinical signs and symptoms like pain during biting, are visible. Longitudinal fracture of endodontically treated teeth are irritating for the patient as well as for the dental health care professional and are most difficult to diagnose.[2]
F-speed conventional and digital radiographic methods (two-dimensional [2D] radiographic images) are insufficient in diagnosing longitudinal fracture. Hence, the diagnosis of vertical root fractures (VRFs) remains a challenge using 2D radiographic images.[5]
When the diagnosis is incorrect, how can the right management be expected? When talking about the right diagnosis, then, future consideration is the prognosis of the root with longitudinal fracture, which is not always good, especially when it extends below the gingival attachment, indicating the extraction of the offending tooth or amputation of the root.[1]
CHALLENGES IN THE TREATMENT OF LONGITUDINAL FRACTURE
Early identification and management an important factors for a good prognosis since restorative intervention can limit the extension of the fracture prevent any microleakage and encroachment of pulpal or periodontal tissues.[1]
Management of different types of longitudinal fractures depends on factors such as the extent of the fracture line and the vitality status of the tooth.[1,6]
The most challenging is the treatment of split tooth involving the pulp chamber. In case of fracture extending to the root, surgical crown lengthening and orthodontic extrusion of the stable fragment can be done, followed by removal of the mobile fragment. Risk factors in such case stay with the site for bacterial infection, leading to bony imperfection.[1]
A long, regular follow-up is required to assess the success of treatment so that any necessary alternation can be done.[1]
BONDING MATERIALS FOR LONGITUDINAL FRACTURE AND FACTORS AFFECTING THE PROGNOSIS OF LONGITUDINAL FRACTURE
Bonding material used for the treatment of longitudinal fracture must possess some desirable properties[7] which are. Factors affecting the prognosis of longitudinal fracture are listed in Table 2.
| Properties of sealing/bonding material |
| It should have an easy application. |
| It should be biocompatible. |
| It should be hydrophilic. |
| It should have a short setting time. |
| It should have bacteriostatic. |
| It should have sufficient fixation strength. |
| Factors affecting the prognosis of longitudinal fracture |
| Periodontal tissue reattachment |
| Regeneration of alveolar bone |
| Proper sealing/bonding of the fracture line |
| Prevention of refracture |
There are different materials used for bonding longitudinal tooth fracture, which are Biodentine, iRoot BP plus, mineral trioxide aggregates, and 4-methacryloxyethyl trimellitate anhydride/methyl methacrylate-tri-n-butylborane (4-META/MMA-TBB), a combination of iRoot BP plus adhesive composite resin, as shown in Table 3.[8-16]
| Biomaterial | Properties | Limitations | Biological effect |
|---|---|---|---|
| Biodentine[8] | • Shorter setting time • Resistant to hydrolysis during setting • More calcium and silicon |
• Mineralizes bone, and dentin stimulates bone growth and mineralization of the dentin • Provides an effective seal against dentin and cementum and promotes biological repair and regeneration of the periodontal ligament |
|
| iRoot BP Plus[9] | • Hydrophilic calcium silicate-based bioceramic material • Excellent sealing ability • Antibacterial and mechanical properties, biocompatible |
• The bond strength between iRoot BP Plus and dentin is not strong | • Repair of pulpal and periodontal tissues’ ability to induce tissue attachment and mineralization |
| MTA[10-13] | • Provides an effective seal against dentin and cementum and don’t need dry conditions | • Long setting time, discoloration, and lower compressive and flexural strength • High-cost |
• Promotes biological repair and regeneration of the periodontal ligament |
| Adhesive composite resin[14] | • Superior adhesive bond strength between adhesive composite resin and dentin | • Poor tissue attachment to the resin surface | • Used in intentional replantation |
| 4-META/MMA-TBB[15] | • A self-cure adhesive resin • Adhesive resin |
• Difficult to control polymerization of the material | • Adheres to cementum by inducing the formation of hybridized cementum |
| Combination of iRoot BP Plus adhesive composite resin[16] | • Biocompatibility and the satisfactory bonding strength | • Bond strength between adhesive composite resin and dentin is strong when holding the fractured segments in position |
MTA: Mineral trioxide aggregates, 4-META/MMA-TBB: 4-methacryloxyethyl trimellitate anhydride/methyl methacrylate-tri-n-butylborane, BP: Bioaggregate putty
RECENT ADVANCES IN THE DIAGNOSIS AND MANAGEMENT OF LONGITUDINAL FRACTURE
Three-dimensional (3D) images like cone-beam computed tomography (CBCT) scan aids in the assessment of anatomical structures that CBCT has been proved accurate in the detection of VRFs as compared to 2D radiographic images, that is, digital and periapical radiographs.[17-19]
With recent advancements in adhesives, fractures once considered irreparable and recommended for extraction can now be successfully restored and reinforced both internally and externally, for example, an intentional replantation method involving the combination of resin and bioceramic material to repair longitudinal fracture through a retention form on both sides of the fracture.[20]
Full coverage restoration can be performed if the fractured segment of the split tooth is stable. For reinforcement of fragments, composite resin, full coverage crown, adhesives, and ligature wires have been done in the literature. Lasers such as carbon dioxide and neodymium-doped yttrium aluminum garnet (NdYAG) used to fuse the fracture segments, and intentional reimplantation has been successfully tried.[20-26]
Apposition of new cement at the fracture site involving the pulpal floor can be done using novel biomaterials.[20]
Vital teeth not involving the pulp can be conservatively managed by a cast gold inlay or full cast crown.[20]
Fractured cusp can be treated by a novel technique known as the matricing and holding technique, which involves the temporary retention of the fractured cusp segment using a matrix band so that there occurs proliferation of granulation tissue and re-attachment of periodontium to the root dentin surface. It prevents pocket formation in the involved root surface area. This temporary retention of the fractured cusp segment is followed by permanent bonded restoration and then removal of tooth fragment during crown preparation.[27]
CONCLUSION
Functional and esthetic outcomes following longitudinal fracture treatment are important considerations in the case of anterior teeth. When talking about the practical utility of the above-mentioned treatment modalities it is still in controversy, and further research is still required. The success of longitudinal fracture depends on its location, direction, extent, prognosis, and treatment modalities available so we cannot rely on one of them; in fact, we have to consider them all.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent was not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using the AI.
Financial support and sponsorship: Nil.
References
- Longitudinal tooth fractures: Findings that contribute to complex endodontic diagnoses. Endod Top. 2007;16:82-111.
- [Google Scholar]
- Vertical root fractures of endodontically treated posterior teeth: A histologic analysis with clinical and radiographic correlates. Swiss Dent J. 2017;127:14-23.
- [Google Scholar]
- Colleagues for excellence-Cracking the cracked tooth code Chicago, IL: American Association of Endodontists; 2008.
- [Google Scholar]
- Comparison of fracture sites and post lengths in longitudinal root fractures. J Endod. 2015;41:159-63.
- [Google Scholar]
- Detection of vertical root fractures using three different imaging modalities: An in vitro study. J Contemp Dent Pract. 2020;21:549-53.
- [Google Scholar]
- Crack lines: The precursors of tooth fractures-their diagnosis and treatment. Quintessence Int. 1983;14:437-47.
- [Google Scholar]
- Factors affecting the in vitro performance of dentin-bonding systems. Japanese Dent Sci Rev. 2012;48:53-60.
- [Google Scholar]
- Biodentine: From biochemical and bioactive properties to clinical applications. G Ital Endod. 2016;30:81-8.
- [Google Scholar]
- iRoot BP Plus promotes osteo/odontogenic differentiation of bone marrow mesenchymal stem cells via MAPK pathways and autophagy. Stem Cell Res Ther. 2019;10:222.
- [Google Scholar]
- Mineral trioxide aggregate applications in endodontics: A review. Eur J Dent. 2020;14:683-91.
- [Google Scholar]
- Mineral trioxide aggregate material use in endodontic treatment: A review of the literature. Dent Mater. 2008;24:149-64.
- [Google Scholar]
- Endodontic treatment of immature tooth-a challenge. J Pre Clin Clin Res. 2020;14:73-9.
- [Google Scholar]
- Influence of different universal adhesives on fracture resistance of endodontically treated teeth. Conserv Dent Endod. 2021;67:2805-15.
- [Google Scholar]
- Treatment of infected root canals with 4-META/MMATBB resin. Hokkaido J Dent Sci. 2017;38:111-21.
- [Google Scholar]
- New approach for the treatment of vertical root fracture of teeth: A case report and review of literature. World J Clin Cases. 2022;10:5816-24.
- [Google Scholar]
- Three dimensions of printing-deleting pitfalls in endodontic practice. J Pre Clin Clin Res. 2023;17:37-41.
- [Google Scholar]
- Role of cone-beam computed tomography in diagnosis of vertical root fractures: A systematic review and meta-analysis. J Endod. 2016;42:12-24.
- [Google Scholar]
- Cone-beam computed tomography for detecting vertical root fractures in endodontically treated teeth: A systematic review. J Endod. 2016;42:177-85.
- [Google Scholar]
- Splinting of longitudinal fracture: An innovative approach. Case Rep Dent. 2016;2016:5083874.
- [Google Scholar]
- Management of vertical fracture-a case report. J Dent Sci Oral Rehabil. 2011;10:34-5.
- [Google Scholar]
- Management of vertically fractured maxillary second molar. J Dent Sci Res. 2010;2:45-50.
- [Google Scholar]
- Long-term observation of fractured tooth roots preserved by adhesion. Adhes Dent. 1995;13:156-70.
- [Google Scholar]
- Treatment of root fracture by CO2 and Nd: YAG lasers: An in vitro study. J Endod. 1996;22:662-7.
- [Google Scholar]
- Novel matricing technique for management of fractured cusp conundrum-a clinician´s corner. J Clin Diagn Res. 2016;10:ZH01-2.
- [Google Scholar]




